
Introduction to Neurofeedback: Training The Brain Like A Muscle.
We've spent decades trying to improve mental performance, sleep, and emotional resilience through external means: medication, therapy, sleep hygiene routines, meditation apps. These things have their place, but there's a less widely known intervention that works from the inside out, something that doesn't add a chemical to the brain or impose a state onto it, but trains the brain to regulate itself and get into optimal states independently. That intervention is called neurofeedback, and the scientific case for it has been quietly building for over half a century.
A Brief History: From EEG to Brain Training
The story begins in 1924, when German psychiatrist Hans Berger first recorded electrical activity from the human brain using an electroencephalogram, or EEG. For the first time, the brain's internal patterns were visible. In the decades that followed, researchers including Lee Edward Travis, Elmer and Alyce Green, Barbara Brown, and Joe Kamiya explored whether those patterns could be observed, understood, and ultimately influenced. The consensus that emerged from this work was a significant one: the brain responds and adapts to feedback. When the brain is presented information about itself, it responds and learns from it.
The figure most directly responsible for modern neurofeedback as we know it is Barry Sterman. In the late 1960s, while studying sleep in cats at UCLA, Sterman discovered something unexpected: cats whose brains had been trained to produce a specific electrical rhythm (which he called the sensorimotor rhythm, or SMR) showed greater neurological stability, better sleep, and resistance to seizures. When he applied the same training logic to humans with epilepsy, the results held. The principle beneath it was straightforward: if you consistently reward the brain for producing a particular pattern, the brain learns to produce it more reliably. That insight became the foundation of clinical neurofeedback.
What Is Neurofeedback?
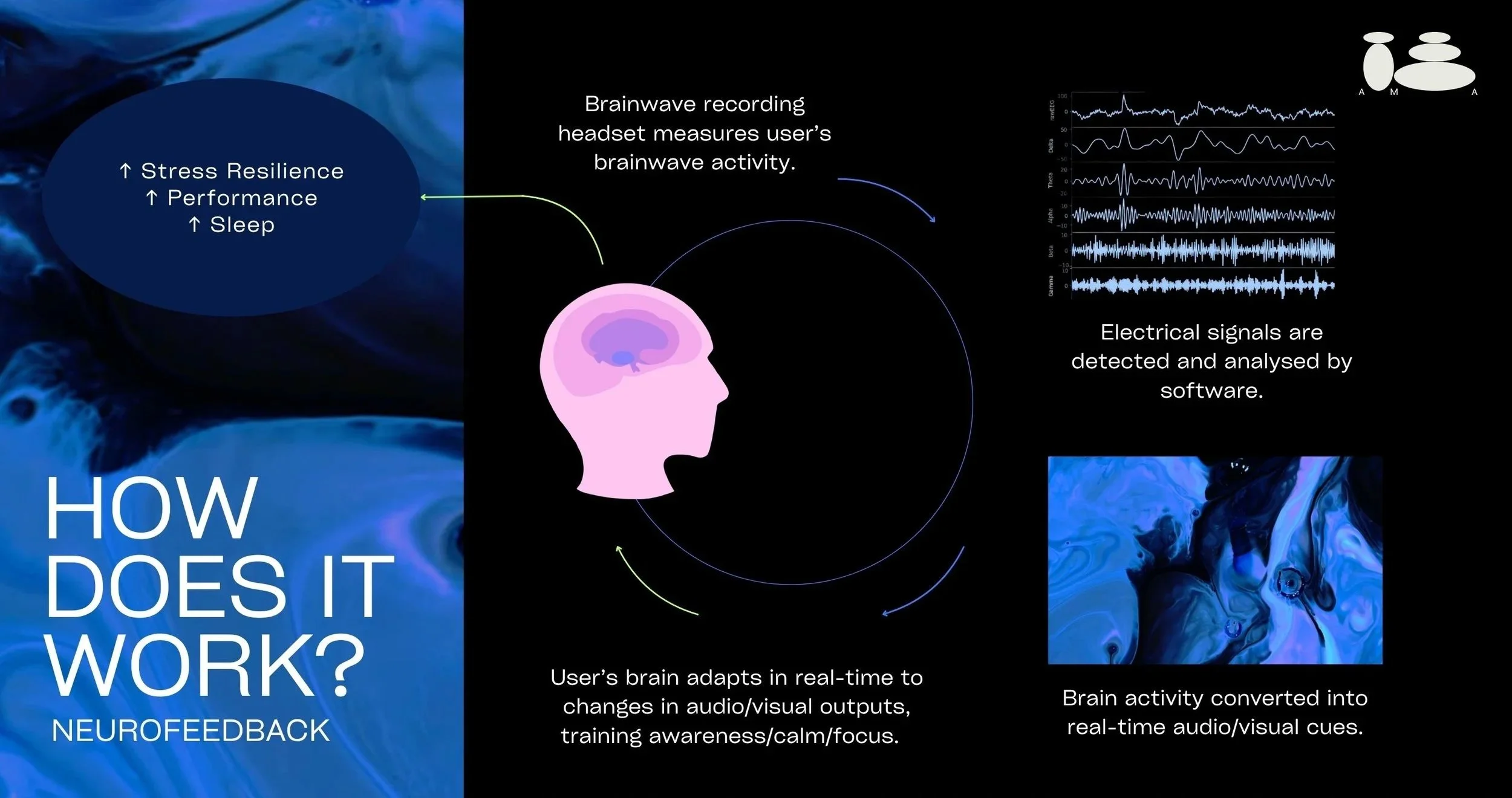
Neurofeedback is a form of brain training built on the principle of operant conditioning, the same mechanism that underlies all learned behaviour. Behaviours that are rewarded tend to increase; behaviours that go unrewarded tend to diminish. In neurofeedback, the behaviour being shaped is a brainwave pattern, and the reward is a real-time audio or visual signal that tells the brain it's doing what you want it to do.
In practical terms, EEG sensors placed on the scalp continuously read the brain's electrical activity. That signal is processed by software, and when the brain produces the target pattern (a frequency associated with calm focus, relaxed attention, or deeper rest, depending on what's being trained) it receives an immediate reward cue: the audio gets louder, the screen brightens. When the brain drifts from that pattern, the feedback stops. Over repeated sessions, the brain learns to orient itself toward the rewarded state, and those patterns gradually become its new baseline, so the brain learns how to get into these optimal states independently.
What makes neurofeedback worth distinguishing from other brain-directed interventions is that it operates through the brain's own learning mechanisms rather than imposing a state from outside. Other technologies like transcranial direct current stimulation or transcranial magnetic stimulation deliver an external signal to the brain; neurofeedback trains the brain to generate the desired state on its own. The goal is lasting self-regulation, not ongoing dependency on a device or a substance. Think of it less like taking a painkiller and more like physiotherapy; the point is to build a capacity that the person carries with them.
What Happens in a Session?
A session begins with electrode placement using the international 10-20 system, a standardised map of scalp positions that allows practitioners to target specific brain regions consistently. The client then sits comfortably, watching a screen or listening to audio, while the EEG reads their brain's live activity across multiple frequency ranges: from slow, deep-rest frequencies through to fast, alert ones. The feedback mechanism is simple by design. The brain doesn't need to consciously understand what it's doing; it simply responds to the reward signal, the same way any learner responds to reinforcement. A typical course of training runs between 20 and 40 sessions for clinical applications, with effects building cumulatively across the programme rather than arriving all at once.
What the Evidence Says: Stress, Anxiety, Depression, and Trauma
The earliest rigorous clinical applications of neurofeedback targeted stress-related conditions, and the foundational literature here remains among the most cited in the field.
Eugene Peniston and Paul Kulkosky's work in 1989 and 1991 used slow-frequency neurofeedback training with combat veterans experiencing PTSD alongside alcohol use disorder. The results were striking across multiple measures: PTSD symptoms reduced significantly, alcohol relapse rates dropped, and personality assessments showed meaningful positive changes. Their protocol, known as alpha-theta training, works by guiding the brain into a deeply relaxed, borderline sleep state, a threshold that trauma researchers have since associated with reduced emotional reactivity and improved integration of difficult experiences.
For depression, D. Corydon Hammond's 2005 review identified a consistent pattern in the brains of people with depression: reduced activity on the left side of the frontal cortex relative to the right, a pattern associated with low mood and reduced motivation. Neurofeedback protocols designed to rebalance this asymmetry showed repeated improvements across multiple studies.
The work of Bessel van der Kolk and Ruth Lanius added important context to why neurofeedback works in trauma populations. Trauma doesn't only leave psychological marks; it changes the way the brain functions, particularly in the regions responsible for emotional regulation, threat detection, and bodily awareness. Neurofeedback offers a way to train those specific systems directly, without requiring the person to verbally process or re-engage with the trauma itself.
A major 2023 review published in the European Journal of Psychotraumatology (Askovic et al.) pooled results from ten controlled studies of neurofeedback in PTSD. Every single study found that neurofeedback outperformed the control condition. In plain terms: across more than 200 participants, those who received neurofeedback showed substantially greater reductions in PTSD symptoms than those who didn't, with an average remission rate of 79.3% in the neurofeedback group. For context, that's a figure that compares favourably with many established treatments, including several pharmaceutical ones.
Which raises a question worth sitting with. Medication for anxiety, depression, and trauma-related conditions plays a legitimate and often necessary role in clinical care. But medication, by design, manages symptoms while it's being taken. Neurofeedback is built around a different premise, that the brain can be trained to regulate itself more effectively and that this change persists once training is complete. A growing number of researchers and clinicians have noted that this positions neurofeedback as a potentially disruptive alternative in the mental health landscape, particularly for patients seeking a longer-term resolution rather than ongoing management. That's not a critique of pharmacology; it's an observation about what neurofeedback is designed to achieve.
The methodological picture is honest rather than perfect. Studies in this field vary in how they design their protocols and measure their outcomes, and running a true double-blind trial in neurofeedback is genuinely difficult when participants can sometimes sense whether they're receiving real or sham feedback. Researchers acknowledge this. But across a field where the evidence has been accumulating for over 50 years, what emerges consistently is clinically meaningful improvement, particularly in populations where conventional treatments have fallen short.

What the Evidence Says: Cognitive Performance
The most substantial evidence base in neurofeedback sits within ADHD research. Martijn Arns and colleagues' meta-analyses in 2009 and 2014 established neurofeedback as a "probably efficacious" treatment for ADHD, a formal designation that placed it alongside cognitive-behavioural therapy in terms of evidence strength for attention and impulsivity outcomes.
The mechanism is well-aligned with what we know about ADHD neurobiology. ADHD brains tend to show too much slow-wave activity in regions associated with attention and executive function, and too little of the faster, more focused activity associated with alertness and control. Neurofeedback protocols targeting this imbalance work by training the brain toward a more regulated pattern, addressing the underlying dynamic rather than compensating for it chemically.
The implications extend well beyond clinical populations. Gruzelier's research with elite musicians and performing arts students found that alpha-theta and SMR neurofeedback training produced measurable improvements in memory, attention, creativity, and composure under pressure in people without any clinical diagnosis. The cognitive benefits are accessible to anyone whose baseline brain activity is underperforming relative to the demands they're placing on it, which, in a chronically stressed, screen-saturated working population, describes a significant proportion of people.
What the Evidence Says: Sleep
Sleep occupies a particular place in the neurofeedback evidence base, partly because Sterman's original findings were themselves sleep findings. The cats trained on SMR didn't just show neurological stability; they showed better sleep architecture, with denser sleep spindles during deep sleep. Sleep spindles matter because they're the brain mechanism most directly associated with memory consolidation and physical restoration during non-REM sleep.
Hoedlmoser and colleagues replicated this in humans in a 2008 placebo-controlled study: SMR training during waking hours produced shorter time to fall asleep, increased sleep spindle density, and improved memory performance in healthy participants. Schabus and colleagues extended this to people with clinical insomnia in 2014, with consistent improvements in subjective sleep quality across the training programme.
The logic of why neurofeedback works for sleep is grounded in the cortical hyperarousal model of insomnia, the idea that many sleep problems are driven by a brain that simply cannot downregulate from an activated state. Where sleep medication sedates the brain into rest, neurofeedback trains it to find that transition on its own. A 2024 meta-analysis by Recio-Rodriguez and colleagues, covering seven randomised controlled trials, found measurable improvements in sleep architecture from neurofeedback training, particularly through protocols targeting the SMR and slower relaxation frequencies.
Sleep, cognition, and stress regulation are not independent systems and neurofeedback that addresses one tends to carry effects into the others. Clients who train for cognitive performance regularly report better sleep; clients who train for anxiety often find their attention sharpens. This isn't a side effect; it reflects the integrative nature of the brain networks being trained.

Left: Neurofeedback in practice; Middle: qEEG assessment setup; Right: Neurofeedback in practice.
Neurofeedback at AMA
At AMA, every neurofeedback programme begins where most practitioners don't start: with the data. Before any training protocol is designed, clients undergo a full quantitative EEG brain map and analysis. This is a direct assessment of the brain's electrical activity across multiple scalp sites, multiple frequency ranges, and multiple states, not a questionnaire or a clinical interview. The analysis identifies the specific patterns driving the client's presenting concerns, whether that's slow-wave activity disrupting attention and energy, elevated high-frequency arousal preventing sleep, frontal asymmetries associated with low mood, or dysregulation in the circuits governing stress response.
From that analysis, a bespoke training protocol is built around the individual's neurological profile. Training is delivered in structured session packages for foundational work, or in an intensive bootcamp format for clients seeking to compress progress into a shorter window. Outcomes are tracked across the specific domains each client presents with: cognitive performance and executive function, sleep quality, anxiety and stress resilience, or trauma symptom reduction. Neurofeedback is a precise tool, and its effectiveness is directly tied to the quality of the assessment that precedes it.
Conclusion
The brain is plastic, not fixed, and capable of meaningful change at any point in the lifespan when given the right conditions. Neurofeedback works by creating those conditions deliberately, using the brain's own learning mechanisms to shift its default patterns in a targeted direction. Across stress regulation, cognitive performance, and sleep, a consistent body of research spanning more than five decades points in the same direction: the brain can be trained, the effects are meaningful, and for many people, this is an intervention they simply haven't had access to yet. That is the gap we aim to close.
References
Arns, M., de Ridder, S., Strehl, U., Breteler, M., & Coenen, A. (2009). Efficacy of neurofeedback treatment in ADHD: the effects on inattention, impulsivity and hyperactivity: a meta-analysis. Clinical EEG and Neuroscience, 40(3), 180–189.
Askovic, M., Soh, N., Elhindi, J., & Harris, A.W.F. (2023). Neurofeedback for post-traumatic stress disorder: systematic review and meta-analysis of clinical and neurophysiological outcomes. European Journal of Psychotraumatology, 14(2).
Hammond, D.C. (2005). Neurofeedback treatment of depression and anxiety. Journal of Adult Development, 12(2–3), 131–137.
Hoedlmoser, K., Pecherstorfer, T., Gruber, G., et al. (2008). Instrumental conditioning of human sensorimotor rhythm (12–15 Hz) and its impact on sleep as well as declarative learning. Sleep, 31(10), 1401–1408.
Peniston, E.G., & Kulkosky, P.J. (1989). Alpha-theta brainwave training and beta-endorphin levels in alcoholics. Alcoholism: Clinical and Experimental Research, 13(2), 271–279.
Recio-Rodriguez, J.I. et al. (2024). Neurofeedback to enhance sleep quality and insomnia: a systematic review and meta-analysis of randomized clinical trials. Frontiers in Neuroscience, 18.
Schabus, M., Heib, D.P.J., Lechinger, J., et al. (2014). Enhancing sleep quality and memory in insomnia using instrumental sensorimotor rhythm conditioning. Biological Psychology, 95, 126–134.
Voigt, J.D. et al. (2024). Systematic review and meta-analysis of neurofeedback and its effect on posttraumatic stress disorder. Frontiers in Psychiatry.